I enjoy reading and writing about healthy living. I also enjoy a Mediterranean-style diet. My blog offers practical tips to help you lose weight, lower cholesterol, and reduce your risk of cardiovascular disease and other chronic diseases.
Vascular ultrasound is a noninvasive test healthcare providers use to evaluate blood flow in the arteries and veins of the arms, neck and legs. Providers use this test to diagnose blood clots and peripheral artery disease. You may also have this test to see if you’re a good candidate for angioplasty or to check blood vessel health after bypass.
What is a vascular ultrasound?
Vascular ultrasound, also called a duplex study, is a noninvasive test. This test shows healthcare providers how blood flows in your arms, neck and legs. High-frequency sound waves create detailed images of soft tissue and blood vessels.
When is a vascular ultrasound performed?
Your healthcare provider may use vascular ultrasound to see how blood flows through your veins and arteries (blood vessels). You may have this test to help your provider diagnose:
Healthcare providers also use vascular ultrasound to check blood flow to organs. You may have this test if you’ve received an organ transplant.
Providers may also order a vascular ultrasound exam to see if you’re a good angioplasty candidate or check blood vessel health after venous disease bypass surgery.
Who performs a vascular ultrasound exam?
An ultrasound technologist performs your vascular ultrasound exam. These technologists have special training in performing ultrasound tests.
How does vascular ultrasound work?
Vascular ultrasound uses high-frequency sound waves to create detailed images. These sound waves pass through your soft tissues and blood vessels. Sound waves create echoes as they pass through tissue and computers turn these echoes into images or videos.
How do I prepare for a vascular ultrasound?
There’s nothing special you need to do to prepare for a vascular ultrasound. Plan to arrive at the facility about 15 minutes before your vascular ultrasound appointment.
You should wear comfortable and loose-fitting clothing and leave any jewelry or valuables at home. Healthcare providers may ask you to change into a hospital gown.
What happens during a vascular ultrasound?
You lie on an examination table. The technologist applies a lubricating gel to your skin in the areas where they will examine your arteries and veins.
The technologist places a special probe called a transducer against your skin. You might feel a little pressure as they move the probe over the area. You may hear your blood flowing as it makes a pulsing or whooshing sound.
What should I expect after the vascular ultrasound?
When the exam is over, the technologist wipes the lubricating gel away. You can return to work or other activities immediately after your exam.
Does vascular ultrasound have any risks or side effects?
Vascular ultrasound is safe. You won’t have any side effects from the exam.
What results do healthcare providers get from vascular ultrasound?
Vascular ultrasound gives your healthcare provider information about how quickly (or slowly) blood flows through your body. This tells your provider if something is blocking a blood vessel (like a blood clot or plaque) or if blood vessels have become narrow.
How long does it take to get results from a vascular ultrasound?
A doctor who specializes in reading and interpreting radiographic images (radiologist) evaluates the images. When the radiologist has completed their review, they send the results to the doctor who ordered your vascular ultrasound.
When should I call my healthcare provider after a vascular ultrasound exam?
You shouldn’t expect any side effects from a vascular ultrasound exam. Let your healthcare provider know if you develop any new or worsening symptoms such as pain or redness in the examined area.
A note from QBan Health Care Services
Vascular ultrasound is a noninvasive test healthcare providers use to determine how blood flows in arteries and veins in your arms, neck and legs. They use this test to diagnose blood clots, narrowed blood vessels, and other vascular health conditions.
A prenatal or pregnancy ultrasound uses sound waves to create a picture of your baby on a screen. Pregnancy care providers use it to check on the health of your baby and detect certain pregnancy complications. Most people have two ultrasounds during pregnancy, but you may have more if your provider feels it’s medically necessary.
What is an ultrasound in pregnancy?
A prenatal ultrasound (or sonogram) is a test during pregnancy that checks on the health and development of your baby. An obstetrician, nurse midwife or ultrasound technician (sonographer) performs ultrasounds during pregnancy for many reasons. Sometimes ultrasounds occur to check on your baby and make sure they’re growing properly. Other times your pregnancy care provider orders an ultrasound after they detect a problem.
During an ultrasound, sound waves are sent through your abdomen or vagina by a device called a transducer. The sound waves bounce off structures inside your body, including your baby and your reproductive organs. Then, the sound waves transform into images that your provider can see on a screen. It doesn’t use radiation, like X-rays, to see your baby.
Even though prenatal ultrasounds are safe, you should only have them when it’s medically necessary. If there’s no reason for an ultrasound (for example, if you just want to see your baby), your insurance company might not pay for it.
Prenatal ultrasounds may be called fetal ultrasounds or pregnancy ultrasounds. Your provider will talk to you about when you can expect ultrasounds during pregnancy based on your health history.
Why is a fetal ultrasound important during pregnancy?
An ultrasound is one of the few ways your pregnancy care provider can see and hear your baby. It can help them determine how far along you are in pregnancy, if your baby is growing properly or if there are any potential problems with the pregnancy. Ultrasounds may occur at any time in pregnancy depending on what your provider is looking for.
What can be detected in a pregnancy ultrasound?
A prenatal ultrasound does two things:
Evaluates the overall health, growth and development of the fetus.
Detects certain complications and medical conditions related to pregnancy.
In most pregnancies, ultrasounds are positive experiences and pregnancy care providers don’t find any problems. However, there are times this isn’t the case and your provider detects birth disorders or other problems with the pregnancy.
Reasons why your provider performs a prenatal ultrasound are to:
Detect problems with your baby’s organs, muscles or bones.
Ultrasound is also an important tool to help providers screen for congenital conditions (conditions your baby is born with). A screening is a type of test that determines if your baby is more likely to have a specific health condition. Your provider also uses ultrasound to guide the needle during certain diagnostic procedures in pregnancy like amniocentesis or CVS (chorionic villus sampling).
An ultrasound is also part of a biophysical profile (BPP), a test that combines ultrasound with a nonstress test to evaluate if your baby is getting enough oxygen.
How many ultrasounds do you have during your pregnancy?
Most pregnant people have one or two ultrasounds during pregnancy. However, the number and timing vary depending on your pregnancy care provider and if you have any health conditions. If your pregnancy is high risk or if your provider suspects you or your baby has a health condition, they may suggest more frequent ultrasounds.
When do you have your first prenatal ultrasound?
The timing of your first ultrasound varies depending on your provider. Some people have an early ultrasound (also called a first-trimester ultrasound or dating ultrasound). This can happen as early as seven to eight weeks of pregnancy. Providers do an early ultrasound through your vagina (transvaginal ultrasound). Early ultrasounds do the following:
Confirm pregnancy (by detecting a heartbeat).
Check for multiple fetuses.
Measure the size of the fetus.
Help confirm gestational age and due date.
Some providers perform your first ultrasound closer to 12 weeks of pregnancy.
20-week ultrasound (anatomy scan)
You can expect an ultrasound around 18 to 20 weeks in pregnancy. This is known as the anatomy ultrasound or 20-week ultrasound. During this ultrasound, your pregnancy care provider can see your baby’s sex (if your baby is in a good position for viewing their genitals), detect birth disorders like cleft palate or find serious conditions related to your baby’s brain, heart, bones or kidneys. If your pregnancy is progressing well and with no complications, your 20-week ultrasound may be your last ultrasound during pregnancy. However, if your provider detects a problem during your 20-week ultrasound, they may order additional ultrasounds.
How soon can you see a baby on an ultrasound?
Pregnancy care providers can detect an embryo on an ultrasound as early as six weeks into the pregnancy. An embryo develops into a fetus around the eighth week of pregnancy.
If your last menstrual period isn’t accurate, it’s possible that it may be too early to detect a fetal heart rate.
Which ultrasound is most important during pregnancy?
All ultrasounds during pregnancy are important. Your pregnancy care provider uses ultrasound to tell them important information about your pregnancy.
What are the two main types of pregnancy ultrasounds?
The two main types of pregnancy ultrasound are transvaginal ultrasound and abdominal ultrasound. Both use the same technology to produce images of your baby. Your pregnancy care provider performs a transvaginal ultrasound by placing a wand-like device inside your vagina. They perform an abdominal ultrasound by placing a device on the skin of your belly.
Transvaginal ultrasound
During a transvaginal ultrasound, your pregnancy care provider places a device inside your vaginal canal (similar to how you place a tampon). In early pregnancy, this ultrasound helps to detect a fetal heartbeat or determine how far along you are in your pregnancy (gestational age). Images from a transvaginal ultrasound are clearer in early pregnancy as compared to abdominal ultrasound.
Abdominal ultrasound
Your pregnancy care provider performs an abdominal ultrasound by placing a transducer directly on your skin. Then, they move the transducer around your belly (abdomen) to capture images of your baby. Sometimes slight pressure has to be applied to get the best views. Providers use abdominal ultrasounds after about 12 weeks of pregnancy.
Traditional ultrasounds are 2D. More advanced technologies like 3D or 4D ultrasound can create better images. This is helpful when your provider needs to see your baby’s face or organs in greater detail. Not all providers have 3D or 4D ultrasound equipment or specialized training to conduct this type of ultrasound.
Your provider may recommend other types of ultrasounds. Examples of additional ultrasounds are:
Doppler ultrasound: This type of ultrasound checks how your baby’s blood flows through its blood vessels. Most Doppler ultrasounds occur later in pregnancy.
Fetal echocardiogram: This type of ultrasound looks at your baby’s heart size, shape, function and structure. Your provider may use it if they suspect your baby has a congenital heart condition, if you had another child that had a heart condition or if you have certain health conditions that warrant taking a closer look at the heart.
How do I prepare for the test?
There’s no special preparation for an ultrasound. Some pregnancy care providers ask that you come with a full bladder and don’t use the restroom before the test. This helps them view your baby better on the ultrasound. You can bring a support person, but bringing children is discouraged as this is an important test that requires complete focus.
You may be asked to change into a hospital gown, but this isn’t usually required for abdominal ultrasounds. If your provider is performing a transvaginal ultrasound in your first trimester, you’ll put on a hospital gown or undress from the waist down.
What should I expect during a prenatal ultrasound?
You’ll lie on a padded examining table during the test. Most ultrasounds occur in a dimly lit room, which helps your ultrasound technician (or sonographer) see the screen. Your sonographer applies a small amount of water-soluble gel to the skin of your belly. The gel doesn’t harm your skin or stain your clothes, but it may feel cold. This gel helps transmit sound waves more efficiently.
Next, the sonographer places a transducer on the skin of your abdomen. The transducer sends sound waves into your body, which reflect off internal structures, including your baby. The sound waves that reflect back create pictures on a screen. Your sonographer uses these images to take important measurements such as your baby’s head circumference and length. You may see them making lines on the screen or clicking a button to “freeze” certain angles.
There’s virtually no discomfort during a prenatal ultrasound. You may feel mild discomfort if you have to pee. The ultrasound test takes about 30 minutes to complete.
If you have a transvaginal ultrasound, the process is only different in that the transducer is inside your vagina and not on your belly.
What should I expect after a pregnancy ultrasound?
If you had an abdominal ultrasound, your sonographer wipes the gel off your belly. They may print off some ultrasound pictures for you to take home with you.
In most cases, your sonographer won’t discuss the results of your test with you. If your obstetrician performs your ultrasound, they may discuss what they see as they go along.
If a sonographer performs your ultrasound, an obstetrician will look at the images, then discuss their findings with you at your next appointment. Most practices schedule your appointment right after your ultrasound so you get your results the same day.
What are the risks of prenatal ultrasounds?
Studies have shown ultrasounds are safe during pregnancy. There are no harmful side effects to you or your baby.
Is it safe to do an ultrasound every month during pregnancy?
While ultrasounds are safe for you and your baby, most major medical associations recommend that pregnancy care providers should only do ultrasounds when the tests are medically necessary. If your ultrasounds are normal and your pregnancy is uncomplicated or low risk, repeat ultrasounds aren’t necessary.
What results do you get on a pregnancy ultrasound?
Your ultrasound results will be normal or abnormal. A normal result means your pregnancy care provider didn’t find any problems and that your baby is growing and developing normally. An abnormal result means your provider noticed something irregular. If they do, your provider will order additional ultrasounds or diagnostic tests to determine if something is wrong.
Occasionally, the ultrasound is incomplete if there’s difficulty seeing all the structures needed for that particular ultrasound. Your baby’s position or movement sometimes makes it difficult to see everything your provider needs to see. If this is the case, you’ll need a repeat ultrasound and they’ll try again.
There are some limitations to ultrasounds, so your provider may not find certain abnormalities until after birth.
What are reasons you need more ultrasounds during pregnancy?
There are several reasons your pregnancy care provider may order additional ultrasounds during your pregnancy. Some of these reasons include:
Problems with your ovaries, uterus, cervix or other pelvic organs.
Your baby is measuring small for their gestational age or your provider suspects IUGR (intrauterine growth restriction).
Normal results on pregnancy ultrasounds can vary. Generally, a normal result means your baby appears healthy and your provider didn’t find any issues.
Why do some pregnancy providers schedule ultrasounds differently?
The number of ultrasounds you’ll have and when you have them can vary between providers. Every practice operates differently and some providers do things differently based on your health history or symptoms.
When does a pregnancy ultrasound determine sex?
Your baby’s sex isn’t visible on an ultrasound until about 18 to 20 weeks. Be sure to tell your pregnancy care provider whether or not you want to know the sex of your baby before your ultrasound.
A note from QBan Health Care Services
An ultrasound during pregnancy can be both exciting and terrifying. Your pregnancy care provider uses ultrasound to get a better idea of how your baby is growing and developing. There are different types of ultrasounds, and the exact timing may vary depending on your provider. Most pregnant people have two ultrasounds — one in the first trimester and one in the second trimester. However, if there’s a potential complication or medical reason for more ultrasounds, your provider will order more as a precaution. Talk to your provider about the ultrasound schedule during pregnancy and what you can expect.
An abdominal ultrasound uses high-frequency sound waves to see structures inside your belly. This test checks the health of your abdominal organs — like your liver, gallbladder and kidneys — and the blood vessels that lead to them.
What is an abdominal ultrasound?
An abdominal ultrasound is a type of imaging test. It uses high-frequency sound waves to create pictures of the organs and blood vessels in your belly (abdomen).
You might hear healthcare providers use the term sonogram. Generally, “ultrasound” refers to the test, and “sonogram” refers to the image the test produces.
Why would a doctor order an abdominal ultrasound?
There are several reasons why a healthcare provider may recommend an abdominal ultrasound. One of the most common is to check on a developing fetus throughout pregnancy. Providers often call this test a prenatal ultrasound.
Ultrasound can also check parts of your digestive system, including your:
Ultrasound uses sound waves you can’t hear to take pictures of soft tissues inside your body. To capture these images, a provider glides a handheld wand (transducer) over your abdomen.
The ultrasound machine sends out high-frequency sound waves that bounce off structures like organs, blood vessels and other soft tissues. A computer receives these signals and uses them to create pictures.
Abdominal ultrasound preparation
Your healthcare provider will give you complete instructions before your ultrasound. Follow their guidelines to ensure the most accurate test results.
Your provider may ask you to stop eating or drinking some hours before your test. In some cases, you may need to drink a specific amount of water right before your test. Or you may not need to prepare at all.
Abdominal ultrasound fasting
Depending on your situation, you might need to fast before your abdominal ultrasound. Having a full (or empty) bladder or stomach can sometimes lead to blurry images. Ask your provider if you should fast before your appointment.
What to expect during the test
For an abdominal ultrasound, you’ll lie on your back on a comfortable table. You’ll need to pull up or remove your shirt or put on a hospital gown.
During the test, a healthcare provider:
Applies gel to your abdomen. This gel may feel cold, but it won’t hurt you or damage your clothes.
Moves the probe over your skin. Your provider gently moves the handheld ultrasound wand over your skin, on top of the gel. They’ll move the wand back and forth until they clearly see the areas in question.
Gives you instructions. The provider performing this test may ask you to turn to one side or hold your breath for a few seconds.
Cleans your skin. They’ll wipe off any remaining gel on your skin.
If your provider wants to study your blood vessels, your test may include Doppler ultrasound. Doppler sound waves detect details of how blood flows inside your blood vessels.
How long do abdominal ultrasounds take?
On average, an abdominal ultrasound usually takes 30 minutes to complete. But it could take more or less time depending on your situation.
Are ultrasounds safe?
Yes, ultrasound is a safe and accurate imaging test. Unlike X-ray imaging, ultrasound doesn’t use radiation (which can cause health issues at high doses). Ultrasound has no known side effects.
When should I know the results?
After your test, a radiologist (doctor who specializes in reading medical images) will review your ultrasound pictures. Then they’ll write a report of their findings and send it to your primary care physician (PCP). In most cases, this takes about one week or less.
Providers sometimes use ultrasound to diagnose potentially life-threatening conditions in an emergency. If your provider suspects an urgent concern, you’ll get results right away.
What should I ask my healthcare provider?
If you need an abdominal ultrasound, here are some questions you may want to ask your provider:
What type of ultrasound do I need?
Will I need any other tests?
How do I need to prepare for my abdominal ultrasound?
When can I expect to get my results?
Can you drink water before an ultrasound of the abdomen?
It depends. Drinking small amounts of water with daily medication is usually OK. But your provider might need you to fast for eight hours before your exam. If you’re not sure, ask your healthcare provider what you need to do in the hours leading up to your appointment.
A note from QBan Health Care Services
If you need an abdominal ultrasound, it’s normal to wonder what to expect the day of your test. Ultrasound imaging is safe and noninvasive. In most cases, it only takes about 30 minutes. Your healthcare provider can talk to you about why you need an ultrasound and what you can expect once you get your results.
Ultrasound is a noninvasive imaging test that shows structures inside your body using high-intensity sound waves. Healthcare providers use ultrasound exams for several purposes, including during pregnancy, for diagnosing conditions and for image guidance during certain procedures.
What is an ultrasound?
Ultrasound (also called sonography or ultrasonography) is a noninvasive imaging test. An ultrasound picture is called a sonogram. Ultrasound uses high-frequency sound waves to create real-time pictures or video of internal organs or other soft tissues, such as blood vessels.
Ultrasound enables healthcare providers to “see” details of soft tissues inside your body without making any incisions (cuts). And unlike X-rays, ultrasound doesn’t use radiation.
Although most people associate ultrasound with pregnancy, healthcare providers use ultrasound for many different situations and to look at several different parts of the inside of your body.
How does an ultrasound work?
During an ultrasound, a healthcare provider passes a device called a transducer or probe over an area of your body or inside a body opening. The provider applies a thin layer of gel to your skin so that the ultrasound waves are transmitted from the transducer through the gel and into your body.
The probe converts electrical current into high-frequency sound waves and sends the waves into your body’s tissue. You can’t hear the sound waves.
Sound waves bounce off structures inside your body and back to the probe, which converts the waves into electrical signals. A computer then converts the pattern of electrical signals into real-time images or videos, which are displayed on a computer screen nearby.
What are the different kinds of ultrasounds?
There are three main categories of ultrasound imaging, including:
Check for congenital conditions (birth defects) in the fetal brain, spinal cord, heart or other parts of its body.
Check the amount of amniotic fluid.
Most healthcare providers recommend an ultrasound at 20 weeks pregnant. This test tracks the fetus’s growth and development during pregnancy. This ultrasound may also show the biological sex of the fetus. Tell your technician if you do or do not want to know the sex.
Your provider may order extra scans to get answers to any questions or concerns, such as the potential for congenital conditions.
Diagnostic ultrasound
Providers use diagnostic ultrasounds to view internal parts of your body to see if something is wrong or not working properly. They can help your provider learn more about what’s causing a wide range of symptoms, such as unexplained pain, masses (lumps) or what may be causing an abnormal blood test.
For most diagnostic ultrasound exams, the technician places the transducer (probe) on your skin. In some cases, they may need to place the probe inside your body, such as in your vagina or rectum.
The type of diagnostic ultrasound you have depends on the details of your case.
Examples of diagnostic ultrasounds include:
Abdominal ultrasound: An ultrasound probe moves across the skin of your midsection (belly) area. Abdominal ultrasound can diagnose many causes of abdominal pain.
Kidney (renal) ultrasound: Providers use kidney ultrasound to assess the size, location and shape of your kidneys and related structures, such as your ureters and bladder. Ultrasound can detect cysts, tumors, obstructions or infections within or around your kidneys.
Doppler ultrasound: This is a special ultrasound technique that assesses the movement of materials, like blood, in your body. It allows your provider to see and evaluate blood flow through arteries and veins in your body. Doppler ultrasound is often used as part of a diagnostic ultrasound study or as part of a vascular ultrasound.
Pelvic ultrasound: A pelvic ultrasound looks at the organs in your pelvic area between your lower abdomen (belly) and legs. Some of the pelvic organs include your bladder, prostate, rectum, ovaries, uterus and vagina.
Transvaginal ultrasound: Your provider inserts a probe into your vaginal canal. It shows reproductive tissues such as your uterus or ovaries. A transvaginal ultrasound is sometimes called a pelvic ultrasound because it evaluates structures inside your pelvis (hip bones).
Thyroid ultrasound: Providers use ultrasound to assess your thyroid, a butterfly-shaped endocrine gland in your neck. Providers can measure the size of your thyroid and see if there are nodules or lesions within the gland.
Transrectal ultrasound: Your provider inserts an ultrasound probe transducer into your rectum. It evaluates your rectum or other nearby tissues, such as the prostate in people assigned male at birth.
Ultrasound guidance for procedures
Providers sometimes use ultrasound to perform certain procedures precisely. A common use of ultrasound is to guide needle placement to sample fluid or tissue from:
Confirming the placement of an IUD (intrauterine device) after insertion.
Lesion localization procedures.
What is the difference between a 3D ultrasound and a 4D ultrasound?
For ultrasounds during pregnancy, the traditional ultrasound is a two-dimensional (2D) image of the fetus. 2D ultrasound produces outlines and flat-looking images, which allows your healthcare provider to see the fetus’s internal organs and structures.
Three-dimensional (3D) ultrasound allows the visualization of some facial features of the fetus and possibly other body parts such as fingers and toes. Four-dimensional (4D) ultrasound is 3D ultrasound in motion. Providers rarely use 3D or 4D fetal ultrasound imaging for medical purposes, though it can be useful in diagnosing a facial or skeletal issue. They do, however, use 3D ultrasound for other medical purposes, such as evaluating uterine polyps and fibroids.
While ultrasound is generally considered to be safe with very low risks, the risks may increase with unnecessary prolonged exposure to ultrasound energy or when untrained users operate an ultrasound machine. Because of this, the U.S. Food and Drug Administration (FDA) advises against getting a 3D ultrasound for non-medical reasons such as for “keepsake” moments or entertainment.
Who performs an ultrasound?
A doctor or a healthcare provider called an ultrasound technician or sonographer performs ultrasounds. They’re specially trained to operate an ultrasound machine properly and safely.
It’s important to always have your ultrasound performed by a medical professional and in a medical facility.
How do I prepare for an ultrasound?
The preparations will depend on the type of ultrasound you’re having. Some types of ultrasounds require no preparation at all.
For ultrasounds of the pelvis, including ultrasounds during pregnancy, of the female reproductive system and of the urinary system, you may need to fill up your bladder by drinking water before the test.
For ultrasounds of the abdomen, you may need to adjust your diet or fast (not eat or drink anything except water) for several hours before your test.
In any case, your healthcare provider will let you know if you need to do anything special to prepare for your ultrasound. They may give you instructions during an appointment or when scheduling your ultrasound. Instructions may also be available in your electronic medical records if you use such a system.
What happens during an ultrasound?
Preparation for an ultrasound varies depending on what body part you’ll have scanned. Your provider may ask you to remove certain pieces of clothes or change into a hospital gown.
Ultrasounds that involve applying the transducer (probe) over your skin (not in your body), follow these general steps:
You’ll lie on your side or back on a comfortable table.
The ultrasound technician will apply a small amount of water-soluble gel on your skin over the area to be examined. This gel doesn’t harm your skin or stain your clothes.
The technician will move a handheld transducer or probe over the gel to get images inside your body.
The technician may ask you to be very still or to hold your breath for a few seconds to create clearer pictures.
Once the technician has gotten enough images, they’ll wipe off any remaining gel on your skin and you’ll be done.
An ultrasound test usually takes 30 minutes to an hour. If you have any questions about your specific type of ultrasound, ask your healthcare provider.
Is an ultrasound painful?
Ultrasounds that are performed externally (over your skin) are generally not painful. You won’t feel the sound waves that ultrasound uses. If you have to have a full bladder for the procedure, it may be uncomfortable. It may also be uncomfortable to lay on the exam table if you’re pregnant.
Ultrasounds that go inside body cavities, such as your vagina or rectum, may be uncomfortable, but they shouldn’t hurt.
Are ultrasounds safe?
Yes, research to date has largely shown ultrasound technology to be safe with no harmful side effects. Ultrasound doesn’t use radiation, unlike some other medical imaging tests, such as X-rays and CT scans.
Still, all ultrasounds should be done by a professional who has training in using this specialized technology safely.
When should I know the results of my ultrasound?
The time it takes to get your results depends on the type of ultrasound you get. In some cases, such as prenatal ultrasound, your provider may analyze the images and provide results during the test.
In other cases, a radiologist, a healthcare provider trained to supervise and interpret radiology exams, will analyze the images and then send the report to the provider who requested the exam. Your provider will then share the results with you or they may be available in your electronic medical record (if you have an account set up) before your provider reviews the results.
What conditions can be detected by ultrasound?
Ultrasound can help providers diagnose a wide range of medical issues, including:
What questions should I ask my healthcare provider about my ultrasound?
If you need an ultrasound, you may want to ask your provider the following questions:
What type of ultrasound do I need?
What should I do to prepare for my ultrasound?
Do I need any other tests?
When should I expect to get test results?
A note from QBan Health Care Services
Ultrasounds are common, safe and effective imaging tests. Make sure you get an ultrasound from a well-trained professional (sonographer) who understands how to use this technology properly. If you have any questions about your specific ultrasound test, talk to your healthcare provider. They’re available to help.
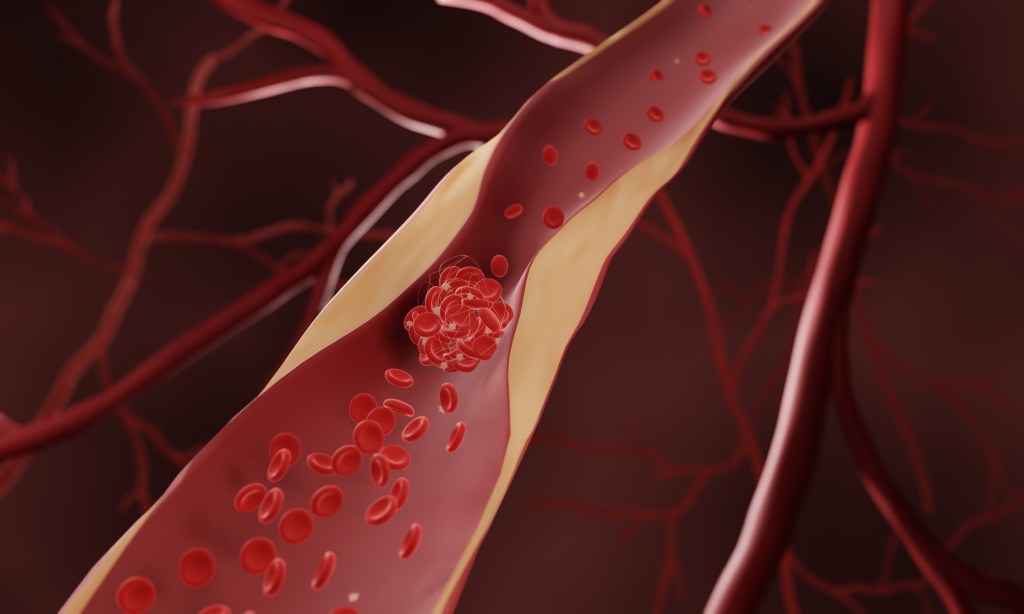
An atheroma (plaque) is a fatty material that builds up inside your arteries. It’s made of cholesterol, proteins and other substances that circulate in your blood. Atheromas grow over time and may lead to coronary artery disease, peripheral artery disease, heart attack or stroke. Lifestyle changes and medications lower your risk of complications.
What is an atheroma?
An atheroma is a fatty substance that builds up in your arteries over time. An atheroma is more commonly known as atherosclerotic plaque, or simply plaque. Atheromas form along the inside lining of your arteries and interrupt blood flow through your body. Atheromas are dangerous because:
They gradually take up more space inside your artery. This leaves less room for blood to flow.
They can rupture and cause a blood clot to form. The clot may block blood flow at that spot. Or, the clot may travel somewhere else in your body and block blood flow there.
Atheromas can lead to complications like a heart attack or stroke. It’s important to learn about what they are and how to lower your risk.
Is atheroma the same as plaque?
Yes. These two words both refer to the fatty substance that lines your artery walls.
What is an atheroma made of?
Atheromas are made of many substances that circulate in your blood. These include:
Calcium is a substance that hardens the atheroma. That’s why people with plaque buildup are known to have “hardening of the arteries.”
What is aortic atheroma?
Aortic atheroma refers to plaque that builds up in your aorta. This condition is called atherosclerosis of the aorta. Your aorta is the largest artery in your body. It extends upward from your heart and then curves downward through your chest and belly. Plaque buildup in your aorta raises your risk of many conditions, including:
No, atheroma isn’t a tumor. It’s a substance that builds up in your arteries.
It can be easy to confuse different medical terms. “Atheroma” looks like the names of some tumors, like carcinoma. But atheroma isn’t related to tumors or cancer. It’s related to your blood vessels and your heart health.
What causes atheromas to form?
Atheromas form because your artery’s inner lining (endothelium) becomes damaged. Scientists continue to learn more about what causes endothelial damage. But it’s clear that once your endothelium is damaged, an atheroma begins to form at the site. And it grows over time.
Risk factors for atheroma formation and growth include:
Atheromas can form anywhere in your arteries. But they’re more likely to form near branch points (where one artery extends from another) or bifurcations (where one artery splits into two).
Think of your arteries like a complex network of roads. Usually, traffic builds up at intersections rather than in areas where the road is wide open with no traffic lights. When it comes to your arteries, plaque usually builds up near the spots where arteries intersect. Scientists continue to study exactly why plaque tends to build up near these intersections.
What is the difference between atheroma and atherosclerosis?
Here’s the short version: Atheroma is a substance, and atherosclerosis is a disease.
Now here’s a bit more detail. Atheroma refers to the fatty material that clogs your arteries. It builds up over time and can lead to complications. Atheroma (plaque) is the defining feature of a disease called atherosclerosis. When you have atherosclerosis, you have plaque buildup in your arteries. The plaque gets bigger slowly and silently over the years.
Plaque buildup can begin when you’re in your teens or 20s, and it continues throughout your life. It’s a result of many factors like diet, lifestyle and genetics. But the process happens more quickly in some people compared with others. And some people face complications earlier in life. This is usually due to risk factors like smoking or a family history of early heart disease.
Atherosclerosis can interfere with blood flow in many different parts of your body. As the atheromas get bigger, they take up more space in your arteries. Over time, this plaque buildup may lead to:
It’s often hard to know if you have plaque buildup since you may not feel any symptoms. In fact, you probably won’t notice symptoms until your arteries are at least 70% clogged. Symptoms depend on which arteries are clogged.
Because atheromas can grow without causing symptoms, it’s important to see your healthcare provider every year. Your provider will talk with you about your risk factors and your family history of heart disease. They may also run tests to check your heart and blood vessels.
Can you reverse atheromas?
Atheromas can’t be reversed once they’ve formed. But there’s a lot you can do to slow down the progression of atherosclerosis. Lifestyle changes and medications play a big role. If you’ve been diagnosed with atherosclerosis, talk with your provider about how to manage your condition.
In general, here are some tips for slowing down atheroma buildup in your arteries:
Don’t smoke or use tobacco products. Tobacco use is a huge risk factor for cardiovascular diseases. Talk with your provider about resources to help you quit.
Eat a heart-healthy diet. Avoid foods high in saturated fat. These include fatty meats and full-fat dairy products. Eliminate any foods containing trans fat (like fast food and packaged convenience foods). Limit your intake of sugar, sodium and refined carbohydrates (like white bread).
Exercise. Aim for 150 minutes of moderate-intensity exercise per week. This could mean you take a 30-minute walk five days per week. Or, find other activities you enjoy, like cycling or swimming. It’s important to check with your provider before starting a new exercise plan.
Take your medications as prescribed. Medications can help you manage risk factors for atherosclerosis. Your provider may prescribe blood pressure medication, cholesterol medication or other drugs. If you experience side effects, talk with your provider right away. Never stop taking a medication without talking to your provider first.
Visit your healthcare provider for yearly checkups. Your provider will assess your risk for atherosclerosis and other cardiovascular diseases. Be sure to keep your follow-up appointments, and share any questions or concerns you have.
A note from QBan Health Care Services
Whether you call it atheroma or plaque, that fatty substance in your arteries isn’t beneficial to your health. But in the battle against atherosclerosis, you’re not alone. Talk with your healthcare provider about ways to slow the progression of plaque buildup in your arteries. Lifestyle changes like quitting smoking and eating healthy foods can help protect your arteries for years to come.
Deep vein thrombosis is a blood clot in a vein located deep within your body, usually in your leg. Get treatment right away so you can prevent serious complications. Treatments include medicines, compression stockings and surgery. Be patient. You may need to take medicine for a few months and wear compression stockings for two years.
What is deep vein thrombosis?
Deep vein thrombosis (DVT, also called venous thrombosis) occurs when a thrombus (blood clot) develops in veins deep in your body because your veins are injured or the blood flowing through them is too sluggish. The blood clots may partially or completely block blood flow through your vein. Most DVTs happen in your lower leg, thigh or pelvis, but they also can occur in other parts of your body including your arm, brain, intestines, liver or kidney.
What is the danger of DVT?
Even though DVT itself is not life-threatening, the blood clots have the potential to break free and travel through your bloodstream. A pulmonary embolism (PE) happens when the traveling blood clots (emboli) become lodged in the blood vessels of your lung. Since this can be a life-threatening condition, you need a quick diagnosis and treatment.
As many as half of those who get a DVT in their legs develop symptoms of intermittent leg pain and swelling that may last months to years. These symptoms are called post-thrombotic syndrome and can happen because of damage to the valves and inner lining of your veins leading to blood “pooling” more than it should. This increases the pressure inside your veins and causes pain and swelling.
Characteristics of this condition include:
Pooling of blood.
Chronic leg swelling.
Increased pressure within your veins.
Increased pigmentation or discoloration of your skin.
Leg ulcers known as venous stasis ulcers.
What is the difference between DVT and a superficial venous thrombosis?
A superficial venous thrombosis (also called phlebitis or superficial thrombophlebitis) is when blood clots develop in a vein close to the surface of your skin. These types of blood clots rarely travel to your lungs unless they move from the superficial system into the deep venous system first. While a physician can diagnose superficial vein clots with a physical exam, they can only diagnose DVT with an ultrasound.
How common is deep vein thrombosis?
Each year, approximately 1 to 3 in every 1,000 adults develop a DVT or pulmonary embolism in the United States, and up to 300,000 people die each year as a result of DVT/PE. It’s the third most common vascular disease, behind heart attacks and strokes. Acute DVT/PE can occur at any age, but are less common in children and adolescents and more common in those over the age of 60. More than half of all DVTs happen as a result of being in the hospital from a medical illness or following surgery. The reason why DVTs are more common after a hospital stay is because you’re lying in bed most of the time instead of moving around like you normally would.
What are the symptoms of deep vein thrombosis?
A DVT usually forms in the veins of your legs or arms. Up to 30%of people with a DVT don’t have symptoms, but sometimes the symptoms are very mild and may not raise concern. The symptoms associated with an acute DVT include:
Swelling of your leg or arm (sometimes this happens suddenly).
Pain or tenderness in your leg or arm (may only happen when standing or walking).
The area of your leg or arm that’s swollen or hurts may be warmer than usual.
Skin that’s red or discolored.
The veins near your skin’s surface may be larger than normal.
Abdominal pain or flank pain (when blood clots affect the veins deep inside your abdomen).
Severe headache (usually of sudden onset) and/or seizures (when blood clots affect the veins of your brain).
Some people don’t know they have a DVT until the clot moves from their leg or arm and travels to their lung. Symptoms of acute PE include chest pain, shortness of breath, cough with blood, lightheadedness and fainting.
It’s important to call your doctor right away or go to the emergency room if you have symptoms of a DVT. Don’t wait to see if your symptoms go away. Get treatment right away to prevent serious complications.
What causes deep vein thrombosis?
These conditions can increase your risk of a deep vein thrombosis:
Having cancer and some of its treatments (chemotherapy).
Having a history of deep vein thrombosis in yourself or your family.
Having limited blood flow in a deep vein because of an injury, surgery or immobilization.
Not moving for long periods of time, like sitting for a long time on trips in a car, truck, bus, train or airplane or being immobile after surgery or a serious injury.
Being pregnant or having recently delivered a baby.
Being older than 40 (although a DVT can affect people of any age).
Your healthcare provider will do a physical exam and review your medical history. You’ll also need to have imaging tests.
Tests to diagnose a DVT
Duplex venous ultrasound. This is the most common test for diagnosing a DVT because it is non-invasive and widely available. This test uses ultrasound waves to show blood flow and blood clots in your veins. A vascular ultrasound technologist applies pressure while scanning your arm or leg. If the pressure doesn’t make your vein compress, it could mean there’s a blood clot. If the results of the duplex ultrasound aren’t clear, your provider can use another imaging test
Venography. In this invasive test, your provider numbs the skin of your neck or groin and uses a catheter to inject a special dye (contrast material) into your veins to see if any blood clots are partially or completely blocking blood flow inside your veins. Venography is rarely used nowadays, but sometimes it is necessary
Magnetic Resonance Imaging (MRI) or Magnetic Resonance Venography (MRV). MRI shows pictures of organs and structures inside your body. MRV shows pictures of the veins in specific locations in your body. In many cases, MRI and MRV can offer more information than a duplex ultrasound or CT scan.
Computed tomography (CT) scan is a type of X-ray that shows structures inside your body. Your provider may use a CT scan to find a DVT in your abdomen, pelvis or brain, as well as blood clots in your lung (pulmonary embolism).
If your doctor thinks you may have a genetic or acquired clotting disorder, you may need to have special blood tests. This may be important if:
You have a history of blood clots that your provider can’t link to any other cause.
You have a blood clot in an unusual location, such as in a vein from your intestines, liver, kidney or brain.
You have a strong family history of blood clots.
You have a family history of a specific genetic clotting disorder.
Activity Guidelines
A DVT may make it harder for you to get around at first because of leg pain and swelling. But you’ll be able to slowly return to your normal activities. If your legs feel swollen or heavy, lie in bed with your heels propped up about 5 to 6 inches. This helps improve circulation and decreases swelling.
In addition:
Exercise your calf muscles if you’re sitting still for long periods of time.
Stand up and walk for a few minutes every hour while awake and especially during a long-haul flight or road trip.
Wear knee-high compression stockings. These minimize leg pain and swelling by at least 50% if you wear them daily.
Avoid activities that may cause a serious injury.
Stay hydrated at all times, and especially during travel.
What treatments are available for people with deep vein thrombosis?
Some people with a DVT may need to be treated in the hospital. Others may be able to have outpatient treatment.
Treatments include medications called anticoagulants (blood thinners), compression stockings and elevating your affected leg(s) at different times throughout the day. In a minority of cases, when the DVT is extensive, invasive treatments (catheter-based procedures) may be required.
The main goals of treatment are to:
Keep the clot from getting bigger and involving other veins.
Prevent the clot from breaking off in your vein and moving to your lungs.
Lessen the risk of another blood clot.
Prevent long-term complications from the blood clot (like chronic venous insufficiency).
Important information about medications
Take your medications exactly as your healthcare provider tells you to.
Have blood tests your provider requests and keep all scheduled laboratory appointments.
Don’t stop or start taking any medication (including medications and supplements you take without a prescription) without asking your provider.
Talk to your provider about your diet. You may need to make changes, depending on the medication you take.
DVT treatments
Anticoagulants (blood thinners)
This type of medication makes it harder for your blood to clot. Anticoagulants also stop clots from getting bigger and prevent blood clots from moving. Anticoagulants don’t destroy or “melt” blood clots. Your body may naturally dissolve a clot, but sometimes clots don’t completely disappear. When they don’t, they usually shrink and become little “scars” inside your veins. Sometimes these “old” clots may result in leg swelling, but oftentimes they don’t cause symptoms.
There are different types of anticoagulants: warfarin, heparin and oral Xa inhibitors. Your doctor will talk to you about the best type of medication for you.
If you need to take an anticoagulant, you may have to take it for only a few months (usually three to six months) or you might take it indefinitely. Your treatment time may be different depending on the specific situations of each individual, including if:
You’ve had clots before.
You’re getting treatment for another illness, like cancer or an autoimmune disease (you may need to take an anticoagulant as long as your risk of a clot is higher.).
Bleeding is the most common side effect of anticoagulants. You should call your doctor right away if you notice that you bruise or bleed easily while taking this medication.
Compression Stockings
You‘ll probably need to wear graded elastic compression stockings to either improve or completely get rid of leg swelling. Damage to the small valves inside your veins often causes this swelling. You may also have swelling because the DVT is blocking blood flow in your vein. You wear most compression stockings just below your knee. These stockings are tight at the ankle and become looser as they go away from your ankle. This causes gentle pressure (compression) on your leg. Some people need to wear these for two years or more. Several clinical studies have shown that compression stockings improve the symptoms of leg pain and swelling by at least 50% as long as they’re worn daily from morning to evening (they don’t have to be worn overnight).
After surgery, your providers may put compression devices on your calves to put pressure on them. These machines squeeze and release the fabric-covered devices around your calves while you’re lying in bed. These devices help prevent a DVT if you’re in the hospital, but they aren’t prescribed outside of the hospital. In addition, unlike compression stockings that you can wear safely when a leg DVT is present, you shouldn’t use these devices for DVT prevention if you have a DVT.
DVT Treatment Procedures
When you can’t take medications to thin your blood or you have blood clots while taking blood thinners without missing doses, a surgeon may have to do a procedure to put in an inferior vena cava (IVC) filter. The procedure is done under local anesthesia. Your surgeon inserts the IVC filter through a catheter into a large vein in your groin or neck, and then into your vena cava (the largest vein in your body). If blood clots in the veins of your legs break off and travel, the IVC filter is designed to prevent large blood clots (emboli) from reaching your lungs and causing a pulmonary embolism. While an IVC filter helps prevent a pulmonary embolism, it doesn’t keep more blood clots from forming in your veins.
How can I reduce my risk?
After you have a DVT, you’ll need to reduce your risk of future DVT/PE clots by:
Taking your medications exactly as your healthcare provider tells you to.
Keeping your follow-up appointments with your doctor and the laboratory. These tell your provider how well your treatment is working.
Making lifestyle changes, such as eating healthier foods, being more active and avoiding tobacco products.
If you’ve never had a DVT, but have an increased risk of developing one, be sure to:
Exercise your calf muscles if you need to sit still for a long time. Stand up and walk at least every half hour if you’re on a long flight. Or get out of the car every hour if you’re on a long road trip.
Get out of bed and move around as soon as you can after you’re sick or have surgery. The sooner you move around, the less chance you have of developing a DVT.
Take medications or use compression stockings after surgery (if your provider prescribes them) to reduce your risk of a clot.
Follow up with your provider as directed and follow their recommendations to reduce your risk of a clot.
What can I expect if I have deep vein thrombosis?
A DVT can take several months to a year to come apart, so you’ll need to keep taking blood thinner medicines as instructed and keep wearing compression stockings until your provider tells you to stop. You may need blood tests to make sure you’re getting the right dose of blood thinners. Your provider may want to do more ultrasounds later to find out if your blood clot is still in the same place, improving or getting larger.
When should I see my healthcare provider?
Tell your healthcare provider if your symptoms aren’t getting better. You should also tell them if you’re bruising too easily or have heavy periods.
When should I go to the ER?
You should get emergency care if the blood thinners you’re taking make you bleed too much, or cause problems like bright red blood in vomit or poop.
What questions should I ask my doctor?
How long will I need to take blood thinners?
When can I travel again?
How often do I need follow-up appointments?
A note from QBan Health Care Services
If you have a deep vein thrombosis, you’re not alone. Every year, at least 1 million Americans get one. Several treatments can help, and your healthcare provider can customize your care to your situation. If they prescribe blood thinners, be sure to keep up with all of your follow-up appointments so you know you’re getting the correct dose.
A pulmonary embolism (PE) is a blood clot from your leg that travels to your lung and stays there. This causes issues with blood flow and oxygen levels in your lungs. Medications can help most people with a pulmonary embolism, but you need a prompt diagnosis and treatment. You’ll need to take medicine for several months afterward.
What is a pulmonary embolism?
A pulmonary embolism (PE) is a blood clot in the blood vessels of your lung. This happens when a clot in another part of your body (often your leg or arm) moves through the veins to your lung. A PE restricts blood flow to your lungs, lowers oxygen levels in your lungs and increases blood pressure in your pulmonary arteries.
Without quick treatment, a pulmonary embolism can cause heart or lung damage and even death.
How serious is a pulmonary embolism?
With proper diagnosis and treatment, a PE is seldom fatal. However, an untreated PE can be serious, leading to other medical complications, including death. About 33% of people with a pulmonary embolism die before they get a diagnosis and treatment.
A pulmonary embolism can:
Cause damage to your lungs.
Cause strain on your heart, causing heart failure.
Be life-threatening, depending on the size of the clot.
How common is a pulmonary embolism?
Pulmonary embolism is one of the most common heart and blood vessel diseases in the world. It ranks third behind heart attack and stroke. In the United States, about 350,000 people a year get a PE.
What are the warning signs of a pulmonary embolism?
The first signs of pulmonary embolism are usually shortness of breath and chest pains that get worse if you exert yourself or take a deep breath. You may cough up bloody mucus.
If you have these symptoms, get medical attention right away. Pulmonary embolism is serious but very treatable. Quick treatment greatly reduces the chance of death.
What are the symptoms of a pulmonary embolism?
Symptoms of pulmonary embolism vary, depending on the severity of the clot. Although most people with a pulmonary embolism experience symptoms, some don’t.
Pulmonary embolism symptoms may include:
Sudden shortness of breath — whether you’ve been active or at rest.
Unexplained sharp pain in your chest, arm, shoulder, neck or jaw. The pain may also be similar to symptoms of a heart attack.
In some cases, feeling anxious, lightheaded, faint or passing out.
Wheezing.
If you have any symptoms of pulmonary embolism, get medical attention immediately.
Because you can have a blood clot and not have any symptoms, discuss your risk factors with your healthcare provider.
What causes a pulmonary embolism?
Pulmonary embolism causes include:
Blood collecting or “pooling” in a certain part of your body (usually an arm or leg). Blood usually pools after long periods of inactivity, such as after surgery or bed rest.
Injury to a vein, such as from a fracture or surgery (especially in your pelvis, hip, knee or leg).
Another medical condition, such as cardiovascular disease (including congestive heart failure, atrial fibrillation, heart attack or stroke).
An increase or decrease in your blood’s clotting factors. Elevated clotting factors can occur with some types of cancer or in some people taking hormone replacement therapy or birth control pills. Abnormal or low clotting factors may also happen as a result of blood clotting disorders.
Who is at risk for a pulmonary embolism?
People at risk of developing a PE include those who:
Ultrasound of your leg. (This helps identify blood clots in people’s legs, or deep vein thrombosis, which can move to the lungs and become a PE and cause more damage.)
A ventilation/perfusion (V/Q) scan, if you’re unable to get contrast for a CT scan. (This is a nuclear scan that can detect clots in your lung.)
Healthcare providers usually treat a PE in a hospital, where they can monitor your condition closely.
The length of your pulmonary embolism treatment and hospital stay will vary, depending on the severity of the clot.
The main treatment for a PE is an anticoagulant (blood thinner).
Depending on the severity of your clot and its effect on your other organs such as your heart, you may also undergo thrombolytic therapy, surgery or interventional procedures to improve blood flow in your pulmonary arteries.
Anticoagulant medications
In most cases, treatment consists of anticoagulant medications (blood thinners). Anticoagulants decrease your blood’s ability to clot. This prevents future blood clots.
As with any medicine, it’s important to understand how and when to take your anticoagulant and follow your provider’s guidelines.
Your diagnosis will determine the type of medication you’ll take, how long you need to take it, and the type of follow-up monitoring you’ll need. Be sure to keep all scheduled follow-up appointments with your provider and the laboratory so they can monitor your response to the medication.
While taking anticoagulants, your follow-up will include frequent blood tests (prothrombin time test) to see how fast your blood clots. This helps your provider know if you’re taking the right dose.
Compression stockings
Compression stockings (support hose) improve blood flow in your legs. People with deep vein thrombosis often use them. You should use them as your provider prescribes. The stockings are usually knee-high length and compress your legs to prevent your blood from pooling.
Talk with your provider about how to use your compression stockings, for how long and how to care for them. It’s important to wash compression stockings according to directions to prevent damaging them.
Procedures
If a PE is life-threatening, or if other treatments aren’t effective, your provider may recommend using surgery or a catheter to remove the blood clot from your pulmonary artery. Thrombolytic therapy (next section) is another option.
Thrombolytic therapy
Thrombolytic medications (“clot busters”), including tissue plasminogen activator (TPA), dissolve the clot. People always receive thrombolytics in the intensive care unit (ICU) of a hospital where a provider can monitor them. You may receive this type of medication if you have a special situation, such as low blood pressure or an unstable condition because of the pulmonary embolism.
Side effects of the treatment
Bleeding is a possible side effect of medications for pulmonary embolism treatment. A provider will give you the dose of anticoagulants or thrombolytics that fits your situation. Keeping you in the hospital allows them to monitor your condition.
How can I prevent a pulmonary embolism?
Ways to prevent a pulmonary embolism include:
Exercise regularly. If you can’t walk around, move your arms, legs and feet for a few minutes every hour. If you know you’ll need to sit or stand for long periods, wear compression stockings to encourage blood flow.
Drink plenty of fluids, but limit alcohol and caffeine.
Don’t use tobacco products.
Avoid crossing your legs.
Don’t wear tight-fitting clothing.
Lose weight if you have overweight.
Elevate your feet for 30 minutes twice a day.
Talk to your provider about reducing your risk factors, especially if you or any of your family members have had a blood clot.
Your provider may also recommend an interventional procedure in which a healthcare provider places a filter inside your body’s largest vein. A vena cava filter traps clots before they enter your lungs.
What can I expect if I have a pulmonary embolism?
Without treatment, a pulmonary embolism is a very serious condition that can lead to permanent illness or death. With treatment, your prognosis depends on the size of the blood clot and blockages, as well as your overall health and how well your heart can pump blood.
Will a pulmonary embolism go away?
It can take months or years for a pulmonary embolism to go away completely. Repeated PE or a very large PE can lead to pulmonary hypertension in some people.
How do I take care of myself?
You’ll need to take a blood thinner for three to six months or longer. Don’t stop taking this unless your provider instructs you to. If you’re taking a blood thinner, don’t do things that have a high risk of an injury that could make you bleed.
Be sure you discuss and understand your follow-up care with your healthcare provider. Follow their recommendations to reduce the risk of another PE.
Keep all appointments with your provider and the laboratory so they can monitor your response to prescribed treatments.
When should I see my healthcare provider?
See your healthcare provider for follow-up appointments. While taking a blood thinner, contact your provider if you have black poop, a bad headache or a bruise that’s getting bigger. These could mean that you’re bleeding.
When should I go to the ER?
Get immediate treatment if you have pulmonary embolism symptoms. (See symptoms section above.)
What questions should I ask my doctor?
What’s the best treatment for me?
How long do I need to take the medicine you prescribe?
When is my first follow-up appointment?
A note from QBan Health Care Services
Treatments help many people with a pulmonary embolism, but it’s important to get a quick diagnosis and treatment. Be on the lookout for symptoms if you have risk factors for a PE and do what you can to prevent one. If you do get a pulmonary embolism, get help quickly.
Blood clots are semi-solid or gel-like masses that form in your arteries and veins. Blood clots help control bleeding, but they may also cause serious medical issues, including deep vein thrombosis, pulmonary embolism and heart attack.
What is a blood clot?
A blood clot is a semi-solid mass of blood cells and other substances that form in your blood vessels. Blood clots protect you from bleeding too much if you’re injured or have surgery. However, you may develop blood clots for other reasons, such as having certain medical conditions. When that happens, blood clots may cause symptoms and can be life-threatening.
What do blood clots do?
Blood clots are the first line of defense if something damages your delicate blood vessels. If you cut yourself from shaving, blood clots are why the bleeding usually stops after a few seconds or minutes.
You can develop a blood clot for other reasons, such as being immobile for a long time or having medical conditions that increase your blood clot risk. When that happens, your blood doesn’t flow as it should.
What are blood clots made of?
Blood clots are made of platelets and fibrin. Platelets are small colorless fragments of cells that your bone marrow makes. Fibrin is a blood protein. It’s sticky and may look like long strings. Platelets and fibrin work together to seal injured areas of your blood vessels.
What do blood clots look like?
A blood clot may look like a clump of reddish jelly held in place with netting. A closer look at a blood clot may show cells that look like tiny plates. These are platelets. The netting is fibrin. Blood clots’ red color comes from red blood cells that are trapped in fibrin as they flow past the injured area.
Where are blood clots located?
You can have a blood clot anywhere in your body. Blood clots that happen in your veins may develop in your arms and legs. This is deep vein thrombosis (DVT). Blood clots that develop in your arteries may appear in your lungs. This is pulmonary embolism. Blood clots that block blood flow to your brain may cause a stroke. Blood clots in your heart may cause a heart attack.
When would I notice a blood clot?
In general, you’d notice blood clot symptoms from clots forming in your veins and arteries. Leg pain, swollen legs and change in skin color may be DVT symptoms. Chest pain or shortness of breath can be symptoms of blood clots in your lungs or heart.
What conditions or disorders involve blood clots?
Blood clot issues are associated with many different kinds of conditions. You may develop a blood clot because you cut yourself and your body is working to stop your bleeding. There are conditions that focus on blood clots, such as bleeding disorders or blood clotting issues. You may also develop conditions that increase your risk of developing blood clots.
Bleeding disorders
If you have a bleeding disorder, it means your blood doesn’t clot as it should and you’re at risk of bleeding uncontrollably if you’re injured. Bleeding disorders include:
Von Willebrand disease: Most people who have von Willebrand disease inherited a mutated gene from one of their biological parents. But von Willebrand disease is also a complication of cancer, autoimmune disorders and heart and blood vessel diseases.
Thrombocytopenia: You may develop thrombocytopenia if you have low platelet counts.
Inherited hemophilia: This condition happens because your body doesn’t make enough clotting proteins to help your blood form clots.
Blood clotting disorders
A blood clotting disorder (hypercoagulable state) is a condition that causes your body to make more blood clots than normal. People may inherit disorders that increase the risk of blood clots or develop disorders during their lifetime. Common blood clotting disorders include:
Factor V Leiden: This inherited disorder is the most common blood clotting disorder. It slightly increases your risk of deep vein thrombosis (DVT) or pulmonary embolism.
Prothrombin Gene Mutation: Like Factor V Leiden, this inherited condition slightly increases your risk of deep vein thrombosis or pulmonary embolism.
Many factors may increase blood clot risk. For example, people with severe coronavirus disease 2019 (COVID-19) have an increased risk. Other factors include:
Age. People age 65 and older have increased blood clot risk.
If you’re born with an inherited (genetic) form of blood clotting disorder, you can’t do anything to prevent the condition or blood clots that happen because of the condition. But you may reduce your risk of developing blood clots by:
Considering non-estrogen alternatives for birth control or hormone therapy.
Staying active.
A note from QBan Health Care Services
Blood clots help control bleeding, whether you’re bleeding from a paper cut, a serious injury or even after surgery. On the other hand, blood clots can also be life-threatening if they keep blood from flowing through your body. Blood clots happen for many reasons, some of which you may not be able to avoid. For example, you may have an inherited (genetic) condition that increases your risk of developing blood clots. If that’s your situation, you’re probably managing your condition with medication and other steps. If you’re worried about developing blood clots, talk to a healthcare provider. They’ll evaluate your overall health and recommend ways you can reduce your risk of developing them.
Peripheral artery disease, or PAD, is an accumulation of plaque (fats and cholesterol) in the arteries in your legs or arms. This makes it harder for your blood to carry oxygen and nutrients to the tissues in those areas. PAD is a long-term disease, but you can improve it by exercising, eating less fat and giving up tobacco products.
What is peripheral artery disease?
Peripheral artery disease (PAD) is plaque buildup in your leg arteries. Your leg arteries carry oxygen and nutrient-rich blood from your heart to your arms and legs. Other names for this are peripheral vascular disease or peripheral arterial disease.
Shaped like hollow tubes, arteries have a smooth lining that prevents blood from clotting and promotes steady blood flow. When you have peripheral artery disease, plaque (made of fat, cholesterol and other substances) forms gradually inside your artery walls. Slowly, this narrows your arteries. This plaque is also known as atherosclerosis.
Many plaque deposits are hard on the outside and soft on the inside. The hard surface can crack or tear, allowing platelets (disc-shaped particles in your blood that help it clot) to come to the area. Blood clots can form around the plaque, making your artery even narrower.
If plaque or a blood clot narrows or blocks your arteries, blood can’t get through to nourish organs and other tissues. This causes damage ― and eventually death (gangrene) ― to the tissues below the blockage. This happens most often in your toes and feet.
PAD can get worse faster in some people more than others. Many other factors matter, including where in your body the plaque forms and your overall health.
How common is peripheral artery disease?
PAD is common, affecting between 8 and 12 million Americans. However, healthcare providers sometimes don’t diagnose or treat PAD enough. Actual numbers are probably higher.
How does peripheral artery disease affect my body?
The typical symptom of PAD is called claudication, a medical term for pain in your leg that starts with walking or exercise and goes away with rest. The pain occurs because your leg muscles aren’t getting enough oxygen.
The dangers of PAD extend well beyond difficulties in walking. Peripheral artery disease increases the risk of getting a nonhealing sore of your legs or feet. In cases of severe PAD, these sores can turn into areas of dead tissue (gangrene) that make it necessary to remove your foot or leg.
What are the stages of peripheral artery disease?
Healthcare providers can use two different systems — Fontaine and Rutherford — to assign a stage to your PAD. The Fontaine stages, which are simpler, are:
I: Asymptomatic (without symptoms).
IIa: Mild claudication (leg pain during exercise).
IIb: Moderate to severe claudication.
III: Ischemic rest pain (pain in your legs when you’re at rest).
IV: Ulcers or gangrene.
What is considered the first symptom of peripheral artery disease?
The first symptom of PAD is usually pain, cramping or discomfort in your legs or buttocks (intermittent claudication). This happens when you’re active and goes away when you’re resting.
What are the typical symptoms of peripheral artery disease?
Symptoms of peripheral artery disease include:
A burning or aching pain in your feet and toes while resting, especially at night while lying flat.
Cool skin on your feet.
Redness or other color changes of your skin.
More frequent skin and soft tissue infections (usually in your feet or legs).
Toe and foot sores that don’t heal.
Half of the people who have peripheral vascular disease don’t have any symptoms. PAD can build up over a lifetime. Symptoms may not become obvious until later in life. For many people, symptoms won’t appear until their artery narrows by 60% or more.
Talk to a healthcare provider if you’re having symptoms of PAD so they can start treatment as soon as possible. Early detection of PAD is important so you can begin the right treatments before the disease becomes severe enough to lead to complications like a heart attack or stroke.
What are the complications of peripheral artery disease?
Without treatment, people with PAD may need an amputation — the removal of part or all of your foot or leg (rarely your arm), especially in people who also have diabetes.
Because your body’s circulatory system is interconnected, the effects of PAD can extend beyond the affected limb. People with atherosclerosis of their legs often have it in other parts of their bodies.
What is the most common cause of peripheral artery disease?
Atherosclerosis that develops in the arteries of your legs — or, less commonly, your arms — causes peripheral arterial disease. Like atherosclerosis in your heart (coronary) arteries, a collection of fatty plaque in your blood vessel walls causes peripheral vascular disease. As plaque builds up, your blood vessels get narrower and narrower, until they’re blocked.
What are the risk factors for peripheral artery disease?
Tobacco use is the most important risk factor for PAD and its complications. In fact, 80% of people with PAD are people who currently smoke or used to smoke. Tobacco use increases the risk for PAD by 400%. It also brings on PAD symptoms almost 10 years earlier.
Compared with nonsmokers of the same age, people who smoke and have PAD are more likely to:
Having kidney disease (both a risk factor and a consequence of PAD).
Although PAD is a different condition from coronary artery disease, the two are related. People who have one are likely to have the other. A person with PAD has a higher risk of coronary artery disease, heart attack, stroke or a transient ischemic attack (mini-stroke) than someone without peripheral artery disease. A person with heart disease has a 1 in 3 chance of having peripheral artery disease in their legs.
Not surprisingly, the two diseases also share some common risk factors. This is because these risk factors cause the same changes in arteries in your arms and legs as they do in your heart’s arteries.
How is peripheral artery disease diagnosed?
A provider will perform a physical exam and review your medical history and risk factors. They may order noninvasive tests to help diagnose PAD and determine its severity. If you have a blockage in a blood vessel, these tests can help find it.
You may also need an invasive test called an angiogram to find artery blockages.
Can peripheral artery disease be reversed?
Yes. Some studies have shown that you can reverse peripheral vascular disease symptoms with exercise and control of cholesterol and blood pressure.
With early diagnosis, lifestyle changes and treatment, you can stop PAD from getting worse. If you think you’re at risk for PAD or may already have the disease, talk to your primary care doctor, vascular medicine specialist or cardiologist so you can get started on a prevention or treatment program right away.
How is peripheral artery disease treated?
Lifestyle changes, medications and procedures can treat PAD.
The two main goals of peripheral artery disease treatments are:
Reducing your risk of cardiovascular events.
Improving your quality of life by easing the pain that occurs with walking.
Lifestyle changes
Treatment of PAD starts with making lifestyle changes to reduce your risk factors. Changes you can make to manage your condition include:
Quit using tobacco products. Ask your healthcare provider about smoking cessation programs.
Eat a balanced diet that’s high in fiber and low in cholesterol, fat and sodium. Limit fat to 30% of your total daily calories. Saturated fat should account for no more than 7% of your total calories. Avoid trans fats, including products made with partially hydrogenated and hydrogenated vegetable oils.
Exercise. Start a regular exercise program, such as walking. Walking can help treat PAD. People who walk regularly can increase the distance they’re able to walk before their legs hurt.
Manage other health conditions, such as high blood pressure, diabetes or high cholesterol.
Keep your stress level low. Exercise, yoga and meditation may help with this.
Practice good foot and skin care to prevent infection and reduce the risk of complications.
Medications
Medicines can help you with conditions such as high blood pressure (antihypertensive medications), high cholesterol (statin medications) and diabetes. These medicines treat the risk factors of PAD and decrease your risk of stroke and heart attack.
Your healthcare provider may prescribe an antiplatelet medication such as aspirin or clopidogrel. They alsomay prescribecilostazol to improve your walking distance. This medication helps people with intermittent claudication exercise longer before they get leg pain.
Supervised exercise programs
A supervised exercise program will improve the symptoms of pain in your legs with walking, allowing you to walk farther. A structured program typically includes walking on a treadmill in a supervised setting at least three times per week.
People with PAD should also walk at home for a total of at least 30 to 60 minutes every day. The usual prescription is called the “Start/Stop” exercise:
Walk until the discomfort reaches a moderate level and then stop.
Wait until the discomfort goes away completely.
Start walking again.
Minimally invasive or surgical treatments
For some people with more severe PAD, leg pain may still cause problems in daily life, even after a few months of exercise and medications. In more severe cases, people need to improve their blood flow to relieve pain at rest or to heal a wound.
More advanced PAD that’s causing severe pain and limited mobility may require endovascular (minimally invasive) or surgical treatment. Some heart disease treatments also treat peripheral artery disease, including:
How long does it take to recover from treatment for peripheral artery disease?
Depending on the treatment you received, you may spend one night or several in the hospital. You may only need a few days to recover from an atherectomy. But you’ll need a week after an angioplasty. It can take six to eight weeks to recover completely from peripheral artery bypass surgery.
How can I reduce my risk of peripheral artery disease?
Knowing that you have risk factors for PAD may motivate you to prevent it. The same advice for keeping your heart healthy applies to caring for your circulation, too:
Manage your weight.
Eat a low-fat, low-sugar diet that includes at least five servings of fresh fruits and vegetables every day.
Don’t use tobacco products.
With your doctor’s approval, exercise for at least 30 minutes a day on most days of the week.
If you have heart disease, you should discuss your risk factors for PAD with your healthcare provider. Report any symptoms you’re having, such as pain, weakness or numbness in your legs.
What can I expect if I have peripheral artery disease?
Like most health conditions, PAD is more treatable when a healthcare provider finds it early. Peripheral vascular disease progresses at different rates. This depends on many factors, including where the plaque formed in your body and your overall health.
Outlook for peripheral artery disease
Peripheral artery disease is a condition you’ll have for the rest of your life. Although there’s no cure for PAD, you can manage it. You can help keep peripheral vascular disease from progressing in several ways:
Not using tobacco products.
Exercising regularly.
Limiting fat and following a healthy diet.
Managing your risk factors, such as diabetes, high cholesterol and high blood pressure.
How do I take care of myself?
It’s important to take good care of your feet to prevent nonhealing sores. Foot care for people who have PAD includes:
Wearing comfortable, appropriately fitting shoes.
Inspecting your legs and feet daily for blisters, cuts, cracks, scratches or sores. Also check for redness, increased warmth, ingrown toenails, corns and calluses.
Not waiting to treat a minor foot or skin problem.
Keeping your feet clean and well moisturized. (Don’t moisturize an area with an open sore.)
Cutting your toenails after bathing, when they’re soft. Cut them straight across and smooth them with a nail file.
In some cases, your healthcare provider may refer you to a podiatrist (foot expert) for specialized foot care ― especially if you have diabetes. A podiatrist can help you with corns, calluses or other foot problems.
When should I see my healthcare provider?
Contact your healthcare provider if you:
Get a bad infection in a sore on your foot. The infection can expand into your muscles, tissues, blood and bones. If your infection is severe, you may need to go to the hospital.
Can’t walk around enough to do normal activities.
Have pain in your legs when you’re resting. This is a sign of poor blood flow.
When should I go to the ER?
Get immediate help if you can’t feel or move your foot or if it looks different from your other foot’s skin color. This means you’ve lost blood flow to your leg without warning.
What questions should I ask my doctor?
Do I need medications to reduce my risk of PAD?
How far should I walk when I start a walking program?
Do I need surgical procedures for peripheral vascular disease?
A note from QBan Health Care Services
You have the ability to prevent peripheral artery disease (PAD) or keep it from getting worse by making lifestyle changes. Keep all of your follow-up appointments with your healthcare provider and vascular specialist, and take the medicines they prescribe for all of your conditions. Knowing the warning signs of PAD complications helps you know when to ask for help, too.
Carotid artery stenosis, also called carotid artery disease, is a condition that can lead to stroke. When you have carotid artery stenosis, a substance called plaque builds up and blocks the normal flow of blood in your artery. One treatment option for carotid artery stenosis is a surgical procedure call endarterectomy.
What is carotid artery stenosis?
Carotid artery stenosis is a condition that happens when your carotid artery, the large artery on either side of your neck, becomes blocked. The blockage is made up of a substance called plaque (fatty cholesterol deposits). When plaque blocks the normal flow of blood through your carotid artery, you’re at a higher risk of stroke. Plaque build-up is called atherosclerosis.
You have two carotid arteries — one on each side of your neck. These are large arteries that bring blood to your brain, face and head. When they’re healthy, these arteries are smooth and open, like a clean pipe that allows the free flow of fluid without anything in the way. Your body’s circulatory system is a network of tubes that carry blood (containing nutrients and oxygen) to all the parts of your body.
You can develop carotid artery stenosis in either of the two arteries in your neck or in both. This condition can worsen over time without medical care, leading to stroke with severe complications that can include death.
How common is carotid artery stenosis?
The prevalence of carotid artery stenosis in the general population is estimated to be as high as 5%. According to the American Stroke Association, stroke ranks fifth on the list of conditions that cause death. Carotid artery stenosis is something that usually happens over time and as you age, the risk for this condition as well as for stroke increases.
What are the causes and risk factors for carotid artery stenosis?
There are several factors that can increase your chance of developing this condition over time. Some of these are factors you can change. Some contribute to and compound other factors:
Carotid artery stenosis can cause a stroke. The kind of stroke that usually happens from carotid stenosis is pieces of plaque (or platelets that form on plaque) travel to your brain. Called “ischemic” stroke, it cuts off blood supply to a portion of your brain. When this blockage is permanent, your brain cells or neurons start to die.
A transient ischemic attack (TIA) is a “mini-stroke” that’s only a temporary blockage of a small brain artery from plaque and/or platelets. For many people, a TIA precedes an ischemic stroke. For these conditions, it’s very important to seek treatment as quickly as possible in order to prevent cell death.
What are the symptoms of a stroke?
The symptoms of a TIA or stroke can include:
Drooping of one side of your face.
Slurred speech or trouble forming words and communicating with others.
Losing vision in one eye with the experience of a dark shade coming down over your field of vision.
Losing feeling on one side of your body.
Losing muscle strength and having weakness on one side of your body.
If you have carotid artery stenosis that hasn’t caused a stroke, you may not notice any symptoms.
How is carotid artery stenosis diagnosed?
Carotid artery stenosis is often diagnosed after you’ve experienced symptoms of a stroke. The symptoms prompt your healthcare provider to thoroughly check for any type of blockage, which can lead to a discovery of carotid artery stenosis. This condition can also be diagnosed after your provider hears an abnormal sound — called a bruit (whistling sound) or murmur — during an exam of your neck with a stethoscope. There are several tests providers use to confirm a diagnosis of carotid artery stenosis and learn more about the size and location of the blockage. These tests can include:
Ultrasound: Also called a duplex ultrasound, this type of test uses sound waves to create an image of your body’s internal structures. An ultrasound is a painless test that is done on top of your skin. An ultrasound is used to see how blood is flowing through your arteries and find any places where the arteries may be blocked or narrowed.
Computed tomography angiography (CTA): Using a CT scanner — a device that uses X-rays to create a detailed image of your internal organs — your provider can take a detailed view of your carotid arteries. During this test, dye is injected into your bloodstream that will help show any blockages on the images. This test may be used on people with pacemakers or stents from other conditions.
Cerebral angiography: This type of diagnostic test involves using a catheter in a minimally invasive procedure to go into your arteries and get a close look at the blockage. Also in this test, your provider injects contrast material directly into your arteries so that they can see the artery details.
Magnetic resonance angiography (MRA): Similarly to a CT scan but without using X-rays, this test provides detailed images of your arteries. It’s a noninvasive imaging test.
How is carotid artery stenosis classified?
During the diagnosis process, your healthcare provider will look to see if you have the condition, how large it is, and where it’s located. Carotid artery stenosis is generally divided into three groupings: mild, moderate and severe. A mild blockage is one that’s less than 50%. This means that less than half of your artery is blocked. A moderate blockage is between 50% and 79%. The most severe classification involves having the majority of your artery blocked — from 80% to 99%.
How is carotid artery stenosis treated?
The main goal of carotid artery stenosis treatment is to halt the progression of the disease. This starts with lifestyle modifications including a healthy diet, exercise and stopping smoking. A daily baby dose of aspirin along with medications that lower blood pressure and cholesterol may also be used.
In more severe cases and or cases causing symptoms of TIA or stroke, your provider may use a surgical procedure called carotid endarterectomy to remove the plaque from the carotid artery through an incision. Alternatively, your surgeon may place a stent through a large needle puncture and ultimately through the blocked artery. This will open the artery up to its proper size while trapping the plaque away from the blood flow between the stent and the wall. A vascular surgeon or specialist determines which of these procedures is best for each person who needs treatment for carotid disease.
Not every carotid stenosis needs surgical or interventional treatment as these procedures themselves come with risk. Surgeons only recommend procedures to people when the risks of severe stenosis and/or stroke become higher than the risk of the procedure.
What’s the outcome of carotid endarterectomy or stenting?
Carotid artery stenosis can be dangerous if it’s not caught and treated quickly. This condition can cause a stroke, which can lead to death or disability. It’s important to know the signs of a stroke and act quickly if you recognize these signs in yourself or someone else. Quick treatment of carotid artery stenosis can be lifesaving. When indicated, the outcomes of surgery and stenting are excellent. Most people recover very quickly with just an overnight hospital stay.
A note from QBan Health Care Services
As you age, your risk of developing carotid artery stenosis increases. The main thing you can do to prevent this condition, and a complication like a stroke, is to maintain a healthy lifestyle. Exercising, eating healthy foods and not smoking are all examples of a healthy lifestyle. Make regular follow-up appointments with your primary care provider and vascular specialist. Talk to your healthcare provider about ways to keep your heart and entire circulatory system healthy.